Psychotropic Medication Consent Form - Hereby give my consent to treatment with this medication. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that once the targeted symptom or behavior is controlled, the usage of. I understand that i may seek additional information, and that i may. ☐ client gives verbal consent, but unwilling or unable to sign. I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives consent to this treatment plan for psychotropic medications. I give my full consent for the use of the medication indicated above.
I agree to notify my practitioner with any changes or problems with my medications. I give my full consent for the use of the medication indicated above. I understand that once the targeted symptom or behavior is controlled, the usage of. Hereby give my consent to treatment with this medication. ☐ client gives consent to this treatment plan for psychotropic medications. ☐ client gives verbal consent, but unwilling or unable to sign. I understand that i may seek additional information, and that i may. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as.
I understand that i may seek additional information, and that i may. Hereby give my consent to treatment with this medication. ☐ client gives consent to this treatment plan for psychotropic medications. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that once the targeted symptom or behavior is controlled, the usage of. I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives verbal consent, but unwilling or unable to sign. I give my full consent for the use of the medication indicated above.
![[TITLE] Understanding Psychotropic Medication A Consent Form for](https://imgv2-2-f.scribdassets.com/img/document/431008273/original/600340a19a/1707448744?v=1)
[TITLE] Understanding Psychotropic Medication A Consent Form for
☐ client gives verbal consent, but unwilling or unable to sign. I give my full consent for the use of the medication indicated above. I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives consent to this treatment plan for psychotropic medications. Hereby give my consent to treatment with this medication.
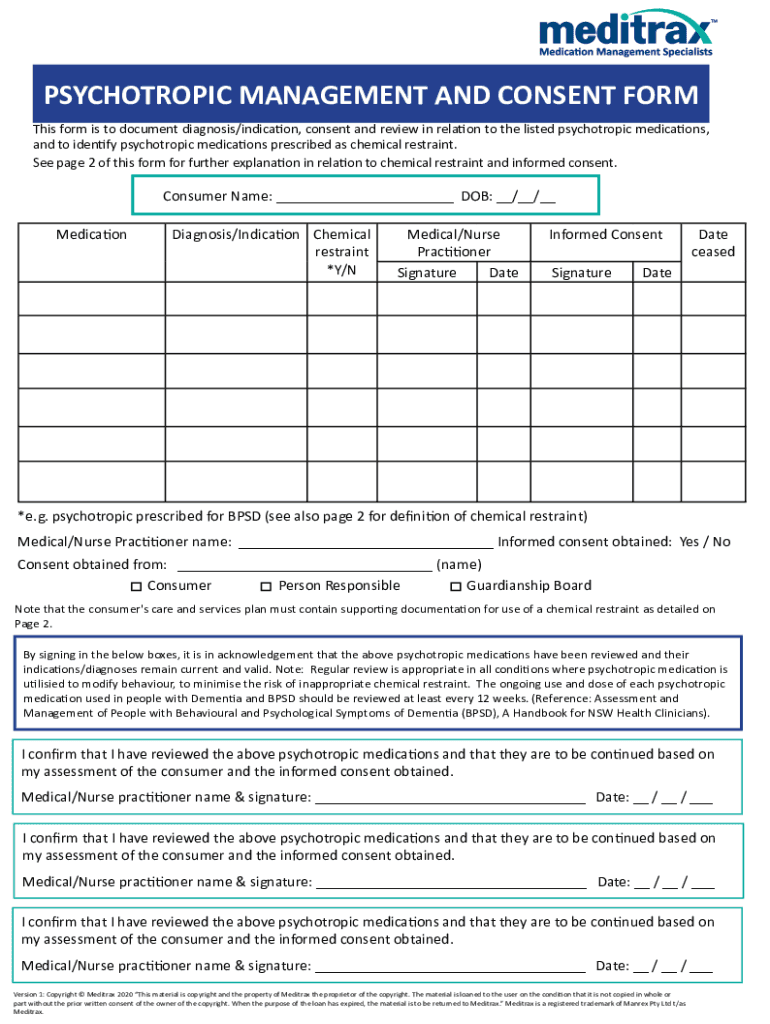
Fillable Online PSYCHOTROPIC MANAGEMENT AND CONSENT FORM Fax Email
☐ client gives consent to this treatment plan for psychotropic medications. Hereby give my consent to treatment with this medication. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that i may seek additional information, and that i may. I give my full consent for the use of the medication.

Psychotropic Medication Consent CF 0173 C 1/15. Psychotropic Medication
I understand that i may seek additional information, and that i may. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives verbal consent, but unwilling or unable to sign. ☐ client gives consent to this treatment plan for psychotropic medications. I give my full consent for the use of.
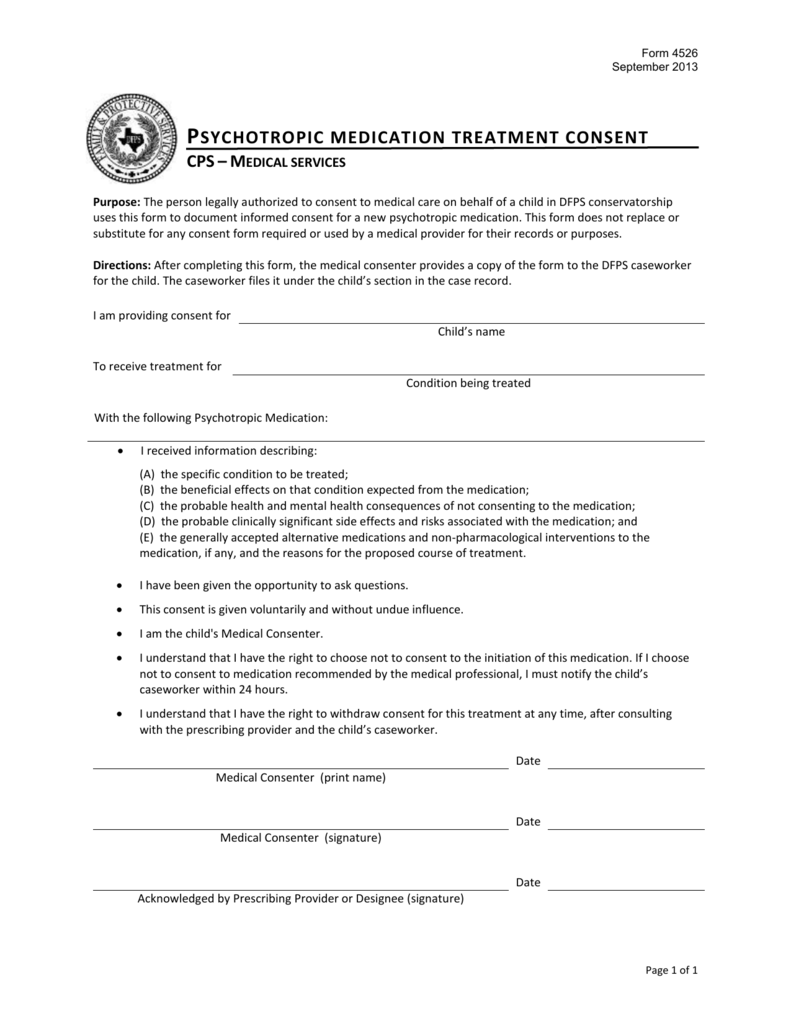
Psychotropic Medication Treatment Consent Form(4526)
I understand that once the targeted symptom or behavior is controlled, the usage of. ☐ client gives consent to this treatment plan for psychotropic medications. I give my full consent for the use of the medication indicated above. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. Hereby give my consent to.
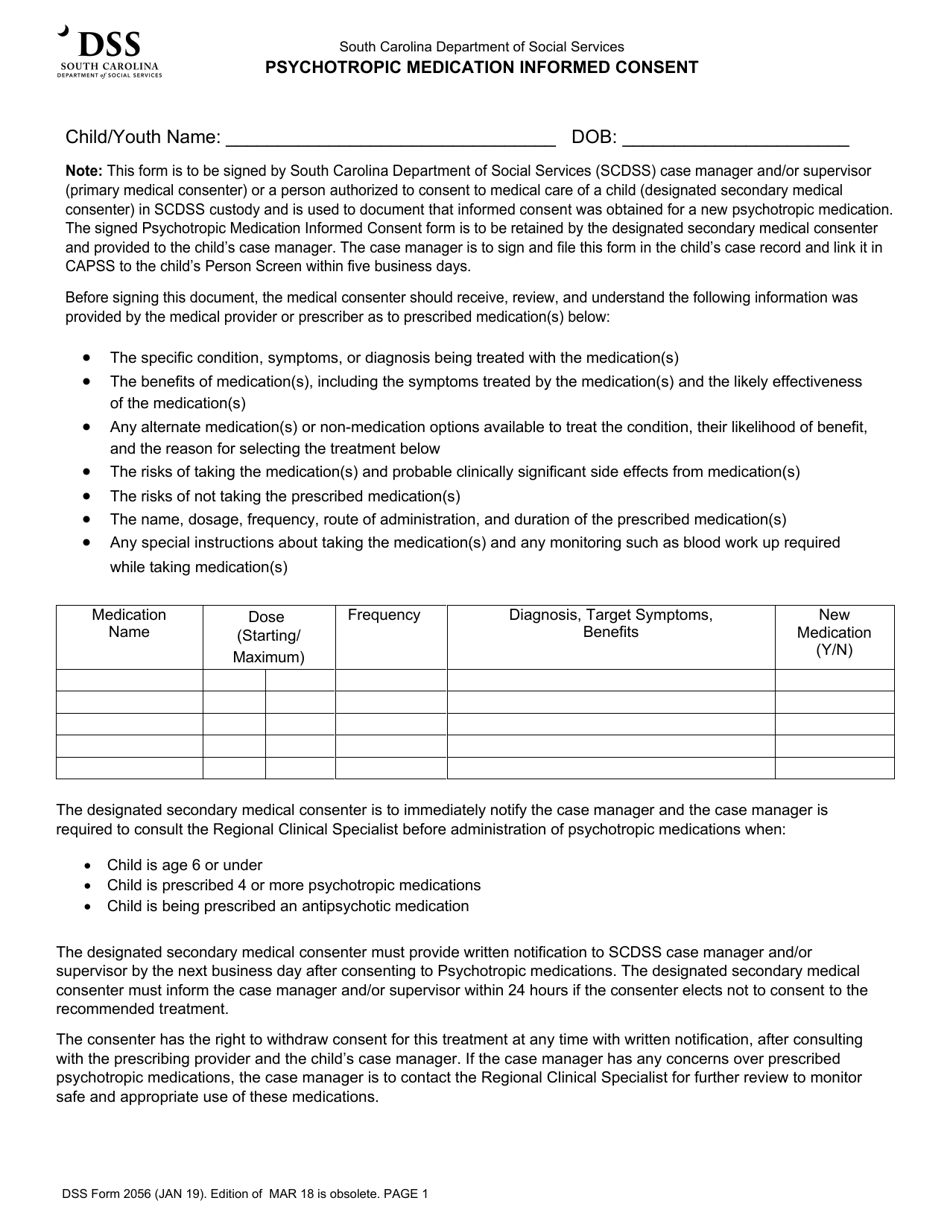
DSS Form 2056 Fill Out, Sign Online and Download Fillable PDF, South
☐ client gives verbal consent, but unwilling or unable to sign. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. Hereby give my consent to treatment with this medication. I understand that once the targeted symptom or behavior is controlled, the usage of. I understand that i may seek additional information, and.

Psychotropic Medication Consent CF 0173 C 1/15 Doc Template pdfFiller
By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives consent to this treatment plan for psychotropic medications. I understand that i may seek additional information, and that i may. I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives verbal consent, but.
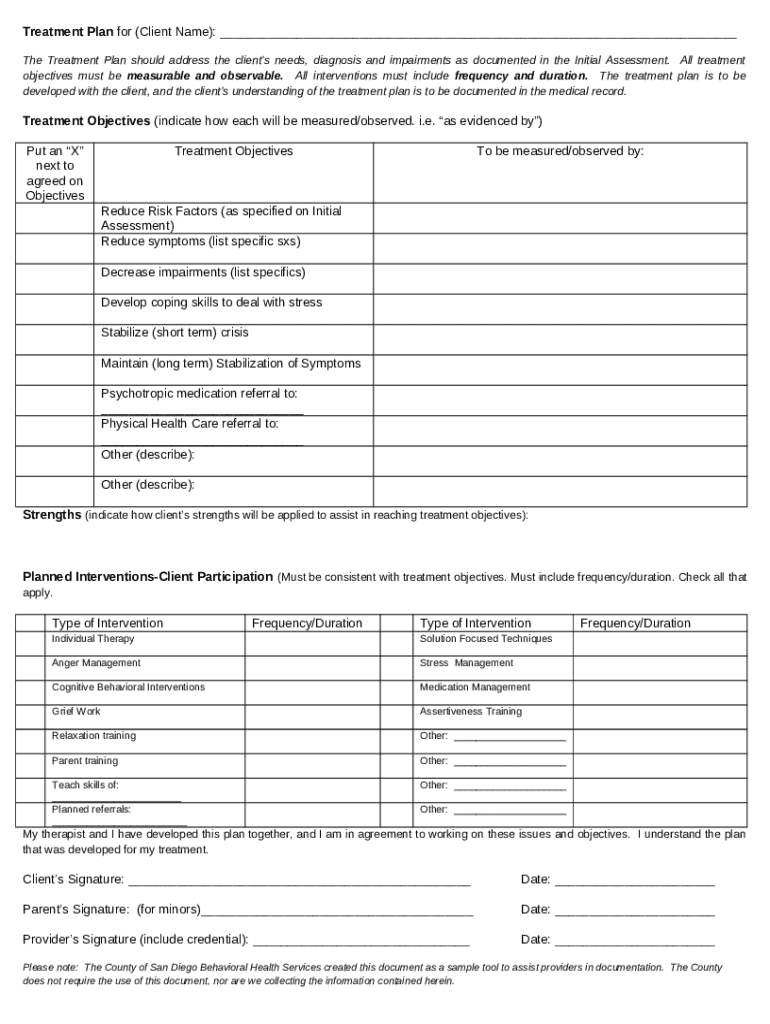
Treatment Plan and Ined Consent for Psychotropic Medical Doc Template
By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that i may seek additional information, and that i may. I understand that once the targeted symptom or behavior is controlled, the usage of. ☐ client gives consent to this treatment plan for psychotropic medications. Hereby give my consent to treatment.

Medication consent Fill out & sign online DocHub
By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives verbal consent, but unwilling or unable to sign. I give my full consent for the use of the medication indicated above. I understand that i may seek additional information, and that i may. Hereby give my consent to treatment with.
Fillable Online Sample Psychotropic Medication Informed Consent Form
I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives consent to this treatment plan for psychotropic medications. Hereby give my consent to treatment with this medication. I understand that i may seek additional information, and that i may. ☐ client gives verbal consent, but unwilling or unable to sign.
Medical Consent Form download free documents for PDF, Word and Excel
I understand that once the targeted symptom or behavior is controlled, the usage of. I understand that i may seek additional information, and that i may. I agree to notify my practitioner with any changes or problems with my medications. I give my full consent for the use of the medication indicated above. By signing below, i give consent for.
I Understand That Once The Targeted Symptom Or Behavior Is Controlled, The Usage Of.
I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives verbal consent, but unwilling or unable to sign. I give my full consent for the use of the medication indicated above. I understand that i may seek additional information, and that i may.
Hereby Give My Consent To Treatment With This Medication.
☐ client gives consent to this treatment plan for psychotropic medications. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as.